To understand abnormal biomechanics of the foot during the human gait cycle, it is important to talk about the normal foot biomechanics, which was covered previously. A variety of problems can occur during the complex gait cycle which can lead to consequences in a runner’s body.
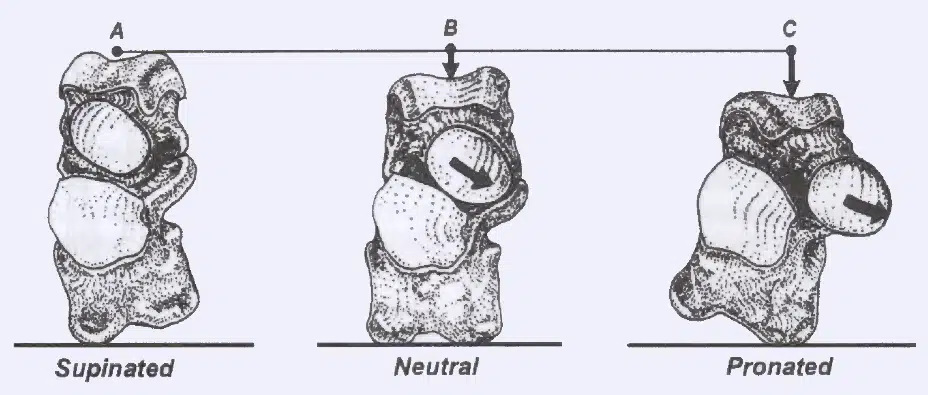
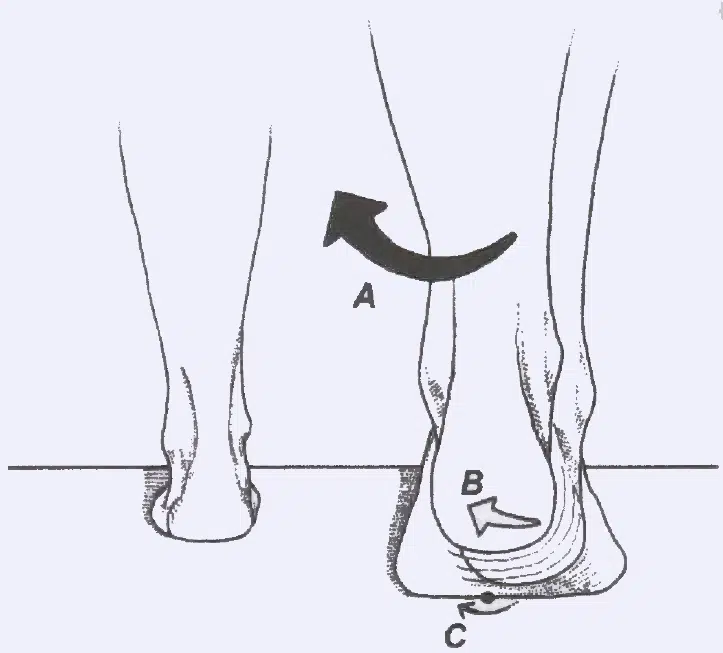
Front view of a right foot – specifically the talus and the calcaneus (heel bone on bottom). Notice the arrows indicating the motion of the talus as it pronates further.
We spoke previously about the motions that the foot goes through that include pronation and supination. Pronation can be generally referred to when the arch collapses or the heel everts, while supination is when the arch rises and the heel returns to neutral or even inverts. One of the most common problems is overpronation or excessive pronation, which occurs in about 90% of the population. There are different degrees of overpronation, where some people drastically drop the arch and can even suction cup the ground with their feet when they walk, whereas others might do it mildly. Approximately 5% of the population over-supinate and the other 5% of the population have “normal” or textbook gait.
But what determines whether you have abnormal foot biomechanics or not? The shape of the joints in a person’s foot can affect whether a person is prone to problems. Each joint in the foot and ankle also has specific minimum ranges of motion that must be present for proper function, and the coordination of movement must be present along with the proper degree of strength, power and endurance. The coordination of movement and muscle strength will be explored in another article.
Articular Pattern
The way that the joints in the foot fit together can be termed articular architecture or pattern. Certain people have feet that have the propensity to be more rigid and other people have feet that have the are more flexible. One of the things that affect this is how the joints fit together. In some cases, people might tend to evert the heel bone. Sometimes you can stand behind somebody who’s barefoot and see that their heel and Achilles tendon seems to be collapsing inward similar to this slash and backslash … / ….
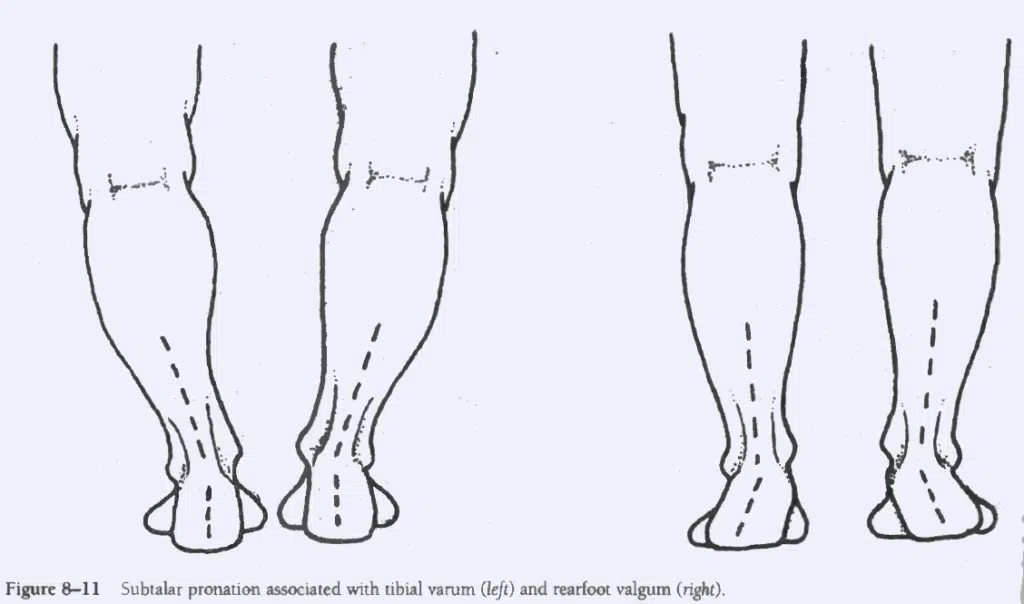
Pronation of the subtalar joint can occur from joint structure, such as tibial varum (bow leggedness) on the left or rearfoot valgum on the right.
When the back of the foot has the tendency to do this type of motion, but the person has a lower arch, it tends to protect joints above the ankle but increases the likelihood that the person will get an injury to the foot or ankle. When an overpronator has a higher arch, eversion of the heel can translate into internal rotation of the leg. This rotation can travel to the knee but often travels all the way up to the hip. This extra motion at the hip must be compensated for which is one thing that can explain why multiple muscles in the hip, including the piriformis and the iliopsoas, are so often tender in overpronators.
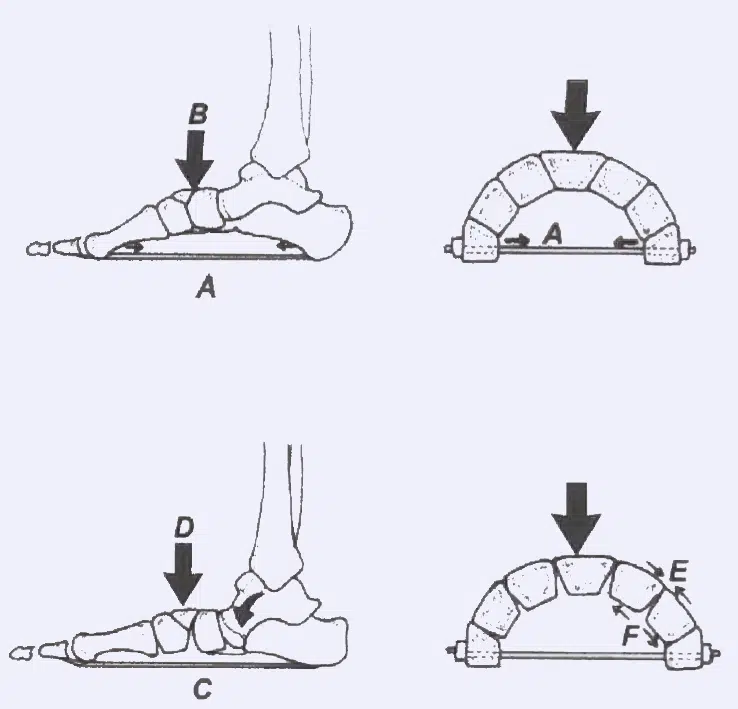
The plantar fascia holds the joints in the foot into an arch shape, that is strong and stable. If a person has a surgical release of the PF, the strength of the arch is lost causing excessive compression at “E” in the image above and tension at “F”.
Because not only the lower leg but the thigh tends to rotate inwards in overpronators, it tends to spare the meniscus of the knee, which can come at the cost of injuries to the patella. The patella has the tendency to be pulled upward but a little laterally during contractions of the quadriceps.
This is because the outside part of the quadriceps tends to be larger and stronger than the inside part of the quadriceps. So not only is the patella being pulled slightly laterally, but the lateral part of the knee is crashing into the patella as it internally rotates. All this motion can also push the shin medially underneath the femur, which stresses the ACL of the knee.
If you will remember, the first ray is the metatarsal and structures that are basically attached to the big toe down in the foot. This first ray must drive down into the ground to help form the main arch (medial longitudinal arch) that people think of in the foot, as well as the transverse arch which goes under the ball of the foot. The first ray that is too mobile and drifts upwards may predispose someone to develop bunion pain, as well as pain under the ball of the foot. Take a look and see whether or not you have a callous in the middle of the ball of your foot.
If you do, this is a sign that your first ray is not driving into the ground and that you do not have a transverse arch. This means that you are pushing off the middle part of your foot, driving the middle heads into the ground instead of the larger bone that is present in the first ray. This can lead to having issues with energy leaks and predispose one to stress fractures in the foot.
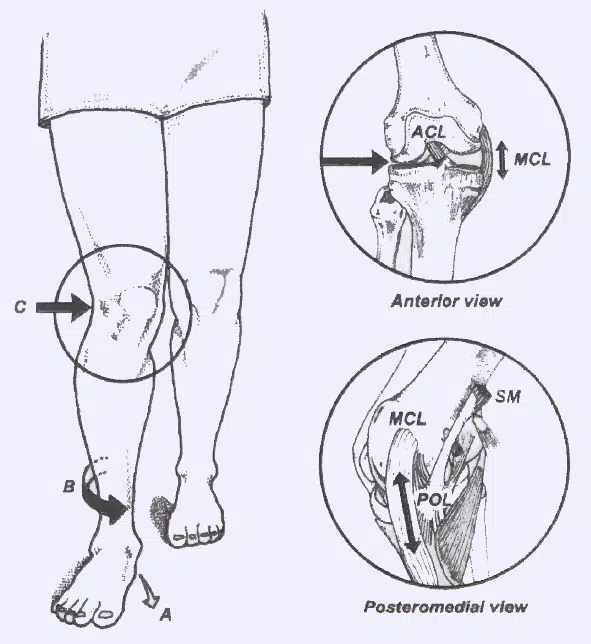
Excessive Pronation is associated with a dropping arch (A), an internally rotated leg (B) and an inward stress on the knee (C). Such an inward (valgus) stress at the knee could damage the medial collateral ligament (MCL) of the knee.
Minimum Range of Motion
In order to have normal function of the joints in the leg, you must have certain ranges of motion at a bare minimum. The function of pointing your toes and feet like a ballerina is called plantar flexion and the opposite movement where you’re bringing your toes closer to your knees is called dorsiflexion. A person who is walking needs to be able to dorsiflex their ankle at least 10° and runners need to be able to get at least 25° of dorsiflexion to avoid abnormal foot biomechanics. This is one of those situations where your body will rob Peter to pay Paul. When a person does not have the minimum range of motion in one joint, it will compensate by stealing the motion in another location. One of the common things that happens for people who do not dorsiflex properly is that the arch can collapse to make up for it, which can seriously strain the plantar fascia. Or the person may make up for it by walking with their foot turned out, so they don’t have to lift up over the toes, which will add compensations up at the hip.
Abductory Twist (above) occurs because of lack of hip extension ROM. It is a compensation.
While this is really geared towards clinicians, it can give you an idea of how problems with the minimum range-of-motion can cause abnormal foot biomechanics. Video quality isn’t great but the information is.
Fixing Abnormal Foot Biomechanics
Treatments for these problems can include a custom foot orthotic, which can be casted at the offices of knowledgeable healthcare providers like podiatrists and chiropractors. Chiropractors often provide custom foot orthotics at a fraction of the price of podiatrists, but you do need to be aware of shoddy products that are made of only foam. While I offer custom foot orthotics in my office, I attempt to stay away from them since I typically use them for temporary support. To be clear, I was trained that orthotics should be eventually removed, just like a person should ultimately give up a crutch when it has outlived its usefulness. However, one crutch that I don’t like and I don’t recommend for people is the plantar fascia night splint and you can see my reasons why by checking out my article. There are other treatment options that seem to provide better long-term relief while building resilience in the individual.
Chiropractic manipulations to the foot and ankle can restore motion that has been lost, leading to a relief of pain. Depending on the issue, static and dynamic stretches can be used to increase the range of motion. Improving muscular coordination, strength, power and endurance will also help to increase a person’s resilience. Graston Technique and Kinesio Taping can also be effective tools at restoring proper motion in the foot as well.
Drawings courtesy of Tom Michaud – Author of Human Locomotion: The Conservative Management of Gait-Related Disorders
You know the feeling. The first mile feels great, but after you put some miles in, a dull ache settles into your lower back. By the time you finish, you're walking a little stiff, wondering if this is just part of getting older or if something's actually wrong. As a...
Stand up for a moment and close your eyes. Notice how your body automatically makes tiny adjustments to keep you upright. You do not have to consciously tell your brain to balance. Your nervous system handles it for you, relying heavily on a structure right at the...
A Lateral Ankle Sprain can happen in a split second. You’re coming down from a rebound during a pickup basketball game, or maybe you simply stepped off a curb wrong while rushing to a meeting. Your foot twists inward, and you feel that familiar, sharp pain on the...
An adductor strain, often called a groin pull, is a common injury that can sideline even the most conditioned athletes. This sharp, sudden pain on the inside of the thigh occurs when the adductor muscles are stretched or torn. While particularly prevalent in sports...
Ankle and foot pain can be a persistent and frustrating problem, often misdiagnosed as more common conditions like plantar fasciitis. When the discomfort involves burning, tingling, or numbness along the inside of your ankle or the bottom of your foot, you may be...
That persistent, nagging pain on the inside of your knee can be a frustrating and confusing problem, which might be pes anserine bursitis. It might show up during your morning run, make climbing a flight of stairs a painful chore, or even ache during a simple walk....